Section1
Recommended TSH Ranges
According to AACE, serum TSH levels should range from 0.45 to 4.12 mIU/L. NACB recommends TSH levels in the blood should be in the range of 0.5 to 2.0 mIU/L. A TSH test can help initially test thyroid function.1-3
Pinch to zoom
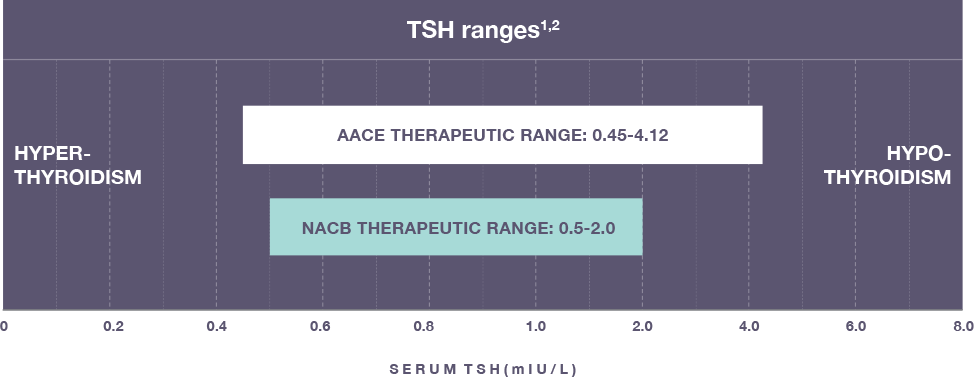
Abbreviations: AACE, American Association of Clinical Endocrinologists; NACB, National Academy of Clinical Biochemistry.
NOTE: Values on horizontal axis are not equal. TSH levels alone may not be diagnostic of a thyroid disorder. Additional laboratory testing and clinical findings may be necessary.